Republished from https://sphweb.bumc.bu.edu/otlt/mph-modules/sb/behavioralchangetheories/BehavioralChangeTheories6.html
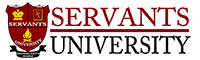
The Transtheoretical Model (also called the Stages of Change Model), developed by Prochaska and DiClemente in the late 1970s, evolved through studies examining the experiences of smokers who quit on their own with those requiring further treatment to understand why some people were capable of quitting on their own. It was determined that people quit smoking if they were ready to do so. Thus, the Transtheoretical Model (TTM) focuses on the decision-making of the individual and is a model of intentional change. The TTM operates on the assumption that people do not change behaviors quickly and decisively. Rather, change in behavior, especially habitual behavior, occurs continuously through a cyclical process. The TTM is not a theory but a model; different behavioral theories and constructs can be applied to various stages of the model where they may be most effective.
The TTM posits that individuals move through six stages of change: precontemplation, contemplation, preparation, action, maintenance, and termination. Termination was not part of the original model and is less often used in application of stages of change for health-related behaviors. For each stage of change, different intervention strategies are most effective at moving the person to the next stage of change and subsequently through the model to maintenance, the ideal stage of behavior.
- Precontemplation – In this stage, people do not intend to take action in the foreseeable future (defined as within the next 6 months). People are often unaware that their behavior is problematic or produces negative consequences. People in this stage often underestimate the pros of changing behavior and place too much emphasis on the cons of changing behavior.
- Contemplation – In this stage, people are intending to start the healthy behavior in the foreseeable future (defined as within the next 6 months). People recognize that their behavior may be problematic, and a more thoughtful and practical consideration of the pros and cons of changing the behavior takes place, with equal emphasis placed on both. Even with this recognition, people may still feel ambivalent toward changing their behavior.
- Preparation (Determination) – In this stage, people are ready to take action within the next 30 days. People start to take small steps toward the behavior change, and they believe changing their behavior can lead to a healthier life.
- Action – In this stage, people have recently changed their behavior (defined as within the last 6 months) and intend to keep moving forward with that behavior change. People may exhibit this by modifying their problem behavior or acquiring new healthy behaviors.
- Maintenance – In this stage, people have sustained their behavior change for a while (defined as more than 6 months) and intend to maintain the behavior change going forward. People in this stage work to prevent relapse to earlier stages.
- Termination – In this stage, people have no desire to return to their unhealthy behaviors and are sure they will not relapse. Since this is rarely reached, and people tend to stay in the maintenance stage, this stage is often not considered in health promotion programs.
To progress through the stages of change, people apply cognitive, affective, and evaluative processes. Ten processes of change have been identified with some processes being more relevant to a specific stage of change than other processes. These processes result in strategies that help people make and maintain change.
- Consciousness Raising – Increasing awareness about the healthy behavior.
- Dramatic Relief – Emotional arousal about the health behavior, whether positive or negative arousal.
- Self-Reevaluation – Self reappraisal to realize the healthy behavior is part of who they want to be.
- Environmental Reevaluation – Social reappraisal to realize how their unhealthy behavior affects others.
- Social Liberation – Environmental opportunities that exist to show society is supportive of the healthy behavior.
- Self-Liberation – Commitment to change behavior based on the belief that achievement of the healthy behavior is possible.
- Helping Relationships – Finding supportive relationships that encourage the desired change.
- Counter-Conditioning – Substituting healthy behaviors and thoughts for unhealthy behaviors and thoughts.
- Reinforcement Management – Rewarding the positive behavior and reducing the rewards that come from negative behavior.
- Stimulus Control – Re-engineering the environment to have reminders and cues that support and encourage the healthy behavior and remove those that encourage the unhealthy behavior.
Limitations of the Transtheoretical Model
There are several limitations of TTM, which should be considered when using this theory in public health. Limitations of the model include the following:
- The theory ignores the social context in which change occurs, such as SES and income.
- The lines between the stages can be arbitrary with no set criteria of how to determine a person’s stage of change. The questionnaires that have been developed to assign a person to a stage of change are not always standardized or validated.
- There is no clear sense for how much time is needed for each stage, or how long a person can remain in a stage.
- The model assumes that individuals make coherent and logical plans in their decision-making process when this is not always true.
The Transtheoretical Model provides suggested strategies for public health interventions to address people at various stages of the decision-making process. This can result in interventions that are tailored (i.e., a message or program component has been specifically created for a target population’s level of knowledge and motivation) and effective. The TTM encourages an assessment of an individual’s current stage of change and accounts for relapse in people’s decision-making process.
